 PDF(564 KB)
PDF(564 KB)
 PDF(564 KB)
PDF(564 KB)
PDF(564 KB)
PDF(564 KB)
狒狒综合征1例
A case of baboon syndrome
 ({{custom_author.role_en}}), {{javascript:window.custom_author_en_index++;}}
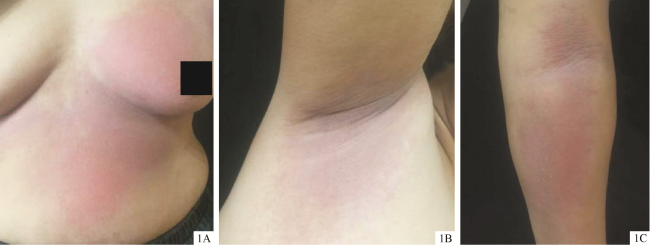
({{custom_author.role_en}}), {{javascript:window.custom_author_en_index++;}}报告1例狒狒综合征。患者女,58岁,因左侧胸腹部、双侧肘窝、腋窝等红斑伴瘙痒4 d就诊。患者5 d前曾接触破碎体温计,既往有含汞成分“红药水”接触过敏史。皮肤科检查: 左侧乳房及左腹部可见大片状鲜红色斑,边界清楚;双侧肘窝、腋窝及腹股沟可见对称分布暗红色斑,边界尚清,压之褪色,触之皮温稍高,未见糜烂、渗出。实验室及辅助检查:血常规,肝、肾功能、血糖及电解质均正常。乙型肝炎表面抗原(HBsAg)(-)、乙型肝炎表面抗体(HBsAb)(+)。心电图检查正常。诊断: 狒狒综合征。予口服依巴斯汀片10 mg,每早1次;盐酸西替利嗪片10 mg,每晚1次;外用炉甘石洗剂(每日4~5次),均用药7 d后停药。治疗第4天时皮损逐渐消退,伴脱屑,8 d后皮损完全消退,部分遗留色素沉着,10 d后色素沉着消退,皮肤恢复正常。目前仍随访中。
A case of baboon syndrome is reported. A 58-year-old woman presented with a 4-day history of pruritic erythematous rashes on the left chest and abdomen, bilateral antecubital fossae, and axillae. The patient contacted a broken thermometer 5 days ago. She also had a history of contact allergy to a mercury-containing topical agent known as ″red medicine″.Dermatological examination revealed a large demarcated fresh patch on the left breast and abdomen. Symmetrically distributed dark red patches with clear boundaries were noticed in the bilateral antecubital fossae, axillae, and groins. The patches were blanched on pressure, and slightly warm could be felt. No erosions or exudation were observed. Laboratory examinations showed normal routine blood tests, liver and kidney function tests, blood glucose, and electrolyte levels. Hepatitis B surface antigen (HBsAg) was negative, while hepatitis B surface antibody (HBsAb) was positive. Electrocardiogram (ECG) was normal. Diagnosis:Baboon syndrome.The patient was treated with oral ebastine tablets (10 mg once daily in the morning), oral cetirizine hydrochloride tablets (10 mg once daily in the evening), and topical calamine lotion (4-5 times daily) for 7 days. The skin lesions gradually subsided on the 4th day of the treatment, accompanied by desquamation, and the lesions completely resolved, with some residual hyperpigmentation by the 8th day. By the 10th day, the skin appeared normal. The patient is still under follow-up.
狒狒综合征 / 汞中毒 {{custom_keyword}} /

| [1] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [2] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [3] |
Hydroxyzine-induced drug eruptions are very rare. We report here a typical case of drug-related Baboon syndrome or symmetrical drug-related intertriginous and flexural exanthema (SDRIFE) which was induced by hydroxyzine in a 60-year-old man. The diagnosis was confirmed by positive patch and oral accidental provocation tests with hydroxyzine. Patch tests and oral provocation tests with cetirizine and levocetirizine were negative. A review of the literature identified only 17 reported cases of hydroxyzine-induced drug eruptions. To the best of our knowledge, we report here the first case of hydroxyzine-induced SDRIFE.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [4] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [5] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [6] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [7] |
杨颜龙, 张素敏, 易松柏, 等. 狒狒综合征1例[J]. 临床皮肤科杂志, 2019, 48(2):114.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [8] |
谷永革, 宋蒙蒙, 卢桂玲, 等. 狒狒综合征1例[J]. 临床皮肤科杂志, 2015, 44(11):727.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [9] |
唐旭华, 周晖, 韩建德, 等. 对称性汞或药物相关的间擦与皱褶疹3例[J]. 中国皮肤性病学杂志, 2016, 30(4):388-390.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [10] |
孔祥君, 卢桂玲, 冯文利, 等. 狒狒综合征并发红皮病1例[J]. 中国皮肤性病学杂志, 2011, 25(10):810-811.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [11] |
李东宁, 王克攀, 王莉丽. 汞相关狒狒综合征一例[J]. 中华皮肤科杂志, 2008, 41(12):841.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [12] |
文利平, 尹佳, 马东来. 汞过敏所致狒狒综合征一例[J]. 中华皮肤科杂志, 2007, 40(10):604-605.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [13] |
韩洁, 李艳佳, 张国强. 汞相关狒狒综合征一例[J]. 中国麻风皮肤病杂志, 2020, 36(1):45-46.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [14] |
朱翊, 郄永涛. 水银引起狒狒综合征一例[J]. 中国麻风皮肤病杂志, 2023, 39(2):124-125.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [15] |
朱青, 张金芳, 宣晓梅, 等. 汞相关狒狒综合征三例[J]. 实用皮肤病学杂志, 2022, 15(6):382-384.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [16] |
于旺, 马秀亮, 刘栋, 等. 狒狒综合征1例[J]. 中国中西医结合皮肤性病学杂志, 2022, 21(4):354-355.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [17] |
付玉萍, 高兴华, 陈国红, 等. 狒狒综合征1例[J]. 实用医学杂志, 2011, 27(8):1332.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [18] |
谭城, 朱文元, 闵仲生, 等. 狒狒综合征[J]. 临床皮肤科杂志, 2007, 36(12):765-766.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [19] |
韩阳, 李晓东, 赵丽萍, 等. 对称性药物相关性间擦部及屈侧疹一例[J]. 实用皮肤病学杂志, 2021, 14(2):112-114.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [20] |
We experienced 15 patients with generalized rash, mostly appearing a day or two after breaking a clinical thermometer or during dental treatment. Similar skin manifestations were revealed, suggestive at first glance of mercury exanthem, i.e. diffuse symmetrical erythema predominantly on major fluxural areas. An inverted triangular or V-shaped erythema on both upper antero-medial thighs was a common feature. Severe cases had miliary pustules and/or purpura on erythematous skin. Pruritus or burning sensation was relatively mild. Pyrexia or malaise was a complaint of more than half the patients. Most of the patients had a previous history of contact dermatitis to Mercurochrome, and by patch-testing were found to have contact allergy to several mercurials, especially inorganic ones. Until recently, Mercurochrome had been most widely used as a topical disinfectant in Japan. This seems to be a possible cause of the high incidence of contact allergy to mercurials in this country. From our findings we feel that our patients had developed systemic contact dermatitis due to inhalation of mercury vapor.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [21] |
The catchword "baboon syndrome" is used to denote a characteristic distribution pattern of systemic allergic contact dermatitis. Diffuse erythema of the buttocks, upper inner surface of the thighs, and axillae are characteristic features. We describe 3 cases provoked by ampicillin, nickel and mercury. The condition may be overlooked and suspected of being a textile dermatitis or seborrhoeic dermatitis of the elderly.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [22] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [23] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [24] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| {{custom_ref.label}} |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
/
| 〈 |
|
〉 |









{kind=link}